How to Order
Contact Us
Wishlist
My Account
Shop
Sensory Motor
Telehealth
Handwriting
Visual Perception
OT/PT Resources
Fine Motor
Brain Breaks
Self Regulation
Speech
Life skills
Yoga for Kids
Motivational Posters
Forms
Webinar
Apparel
Handouts
Gift Cards
⭐ Action Toolkit
Sale
Free Stuff
Blog
Email Newsletters
Click to open the search input field
Click to open the search input field
Search
Menu
Menu
Pediatric Occupational Therapy and Physical Therapy Resources, Forms and Handouts
You are here:
Home
1
/
Pediatric Occupational Therapy and Physical Therapy Resources, Forms and...
School Based Occupational Therapy Screening Form Checklist
$
1.99
Calming Strategies for the Classroom
$
4.99
Occupational Therapy Fine Motor Baselines
$
5.99
Visual Supports: Schedules, Self-Regulation, & Classroom Inclusion
$
7.99
Fine Motor Skills Assessment for OT
$
12.25
School Based Physical Therapy Checklist
$
1.99
Self Regulation Triggers and Calming Tools
$
6.00
Self Regulation Skills Curriculum – Move Work Breathe
$
25.00
Handwriting Rubrics
$
7.99
Breathing Breaks Deep Breathing Exercises
$
5.00
Data Tracking Forms for School Based Occupational and Physical Therapy
$
11.99
Executive Functioning Strategies for Students
$
12.99
Typical Classroom Sensory-Based Problem Behaviors & Suggested Therapeutic Interventions
$
19.95
25 Tip Sheets for School Based Therapists
$
8.99
IEP Goals Related to the Common Core for OT/PT
$
19.95
Emotional Regulation Worksheets – For Boys and Girls
$
14.99
Therapeutic Play Activities for Children
$
24.95
Life Skills Checklists
$
8.99
The Core Strengthening Exercise Program
$
15.99
Self-Assessments and Checklists for Good Work Habits
$
5.99
Daily Routine Visual Schedules
$
4.99
Emotional Regulation Bingo Game
$
6.99
How to Get Organized Worksheets for Students
$
2.99
The Core Strengthening Handbook
$
18.99
What? Why? and How? Series 4 – Visual Skills
$
4.99
The Busy Therapist Bundle
$
46.83
Keyboarding Rubrics
$
7.99
Calm Down Cards
$
4.99
Self-Regulation Flash Cards – Updated
$
14.99
Life Skills of the Month
$
5.99
Mobility Rubrics
$
5.99
How to Write IEP Goals Workbook
$
11.99
2021 Subscription – Your Therapy Source Digital Magazine
$
29.00
Student Self-Regulation Rubrics
$
9.99
Too Slow, Just Right or Too Fast – Visual Supports for Self-Regulation
$
5.00
Emotions Packet
$
4.99
Progress Monitoring Forms – Fine Motor Skills
$
9.99
Sensory Behaviors Checklist
$
7.00
What? Why? and How? Series 3
$
4.99
Cardio Aerobic Exercises for Small Spaces
$
5.99
Sensory Path for School and Home DIGITAL version Sensory Stops
$
19.00
Teaching Catching, Throwing and Kicking Skills
$
7.99
The Hand Strengthening Handbook
$
18.99
School and Home Communication Forms for Therapists
$
5.99
Body Scan Meditation for Kids
$
5.99
Calming Tools, Gross Motor Skills, & Breath Regulation – Animal Walks Bundle
$
7.99
What? Why? and How? Series 1
$
3.99
Sort and Match Emotions and Self Regulation Strategies SEL Activity
$
5.00
IEP Goals Related to the Common Core for OT/PT Grades 3-5
$
19.95
Cut and Paste Sensory Diet
$
9.99
Planning, Time Management, and Organization Skills Bundle
$
29.97
Working Memory, Hemisphere Integration and Attention Building Bundle
$
39.99
Assistive Technology, Classroom Implementation Strategies & Resource Recommendations for Kids Who Struggle to Write
$
19.95
Fantastic Fingers® Fine Motor Program
$
45.00
5 4 3 2 1 Grounding Technique – Stay Calm
$
5.99
Developmental Milestones Handout Pack
$
5.99
Occupational Therapy Preschool Screening
$
6.50
Interoception Body Chart Check
$
5.00
Play – Move – Develop
$
13.95
–
$
24.95
Price range: $13.95 through $24.95
Balance Exercises for Kids
$
5.00
My Goal Tracker – Student Generated Data Collection
$
3.99
What? Why? and How? Series 2
$
4.99
Effective Sensory Integration Session Planbook
$
7.00
Rubrics and Checklists for Pediatric Occupational and Physical Therapy
$
62.90
25 MORE Tip Sheets for School Based Therapists
$
8.99
Sensory Tools for the Classroom – Handouts, Forms and Data Collection
$
5.00
2022 Subscription – Your Therapy Source Digital Magazine
$
39.00
Modifications and Interventions for School Reporting Forms
$
16.95
Visual Supports for Occupational Therapy
$
8.49
Self-Regulation Activity – “Just Right” Train
$
4.99
School Based Therapy Collection 50% Off
$
42.89
The Infant and Toddler Handbook
$
9.99
Heavy Work Sensory Activities Packet
$
7.00
Progress Monitoring Forms – Gross Motor Skills
$
7.99
Handwriting Problem Solutions Resource Guides BUNDLE
$
29.95
Therapeutic Food Survey
$
4.00
School Based Therapy Planner 2022 2023
$
11.99
Teen Self-Regulation and Emotions Adapted Book
$
5.00
What? Why? How? Series 1-4 Handout Collection
$
13.27
Self Calming Strategies
$
3.99
Functional Handwriting and Typing Task Analysis
$
5.00
Emotion Check In Packet
$
5.00
Proprioceptive Poems – Movement Poems
$
4.99
Taming Idiopathic Toe Walking: A Treatment Guide for Parents and Therapists
$
29.95
Therapeutic Activities for Home and School
$
16.95
Data Collection for Special Education Templates – EASY
$
9.99
Dressing Skills Rubrics
$
5.99
Resistance Band Exercises for Kids
$
7.50
Size of the Problem Visual Supports and Activities
$
6.00
VAMPS Assessment Visual Activity, Motor, Postural, & Sensorimotor Assessment
$
39.95
Sensory Choice Boards
$
7.00
Occupational Therapy Milestones Checklist – Ages 2 to 6
$
12.50
Visual Supports for Physical Therapy
$
5.99
Even 35 MORE Tip Sheets for School Based Therapists
$
9.99
Impulse Control Workbook – Pause, Think, Act
$
17.00
PT or OT Session Note Google Form with Schedule
$
2.99
Taming Idiopathic Toe Walking AND Toe Walking Observation Screening Tool Discounted Bundle
$
36.90
The Handwriting Book – FSFK Team
$
15.99
All About Me Glyphs
$
5.00
Digital Magazine 2024 Your Therapy Source Subscription
$
49.00
School Based Physical Therapy Forms
$
13.95
–
$
19.95
Price range: $13.95 through $19.95
Feelings Activities
$
2.49
Rainbow Mindfulness and Movement Packet
$
10.00
Student Planner PDF – Forms and Lists
$
9.95
The Hand Strengthening Exercise Program
$
15.99
Personal Hygiene Rubrics
$
5.99
Teaching Motor Skills to Children with Cerebral Palsy and Similar Movement Disorders – A Guide for Parents and Professionals
$
19.95
Writing Measurable Sensory Goals
$
5.00
Yoga Lesson Plan – I Can Slow Down
$
10.00
Growth Mindset Curriculum: Discussion Guide, PowerPoint /Posters, & Activities
$
6.99
Winter Mindfulness and Movement Activity
$
7.00
Telehealth Occupational Therapy Evaluation Report Template – Pediatric/ School-Based
$
20.00
The Amazing Brain Workbook for Kids
$
17.00
Study Skills and Student Homework Planner
$
7.00
Handouts for Pediatric Therapists, Parents, and Teachers
$
24.99
The Practical Guide to Toilet Training the Autistic Child
$
26.99
Occupational Therapy Reminders: Handwriting, Organization and Scissor Skills
$
4.99
Forms for Functional Writing Practice
$
5.00
Pediatric Occupational Therapy Telehealth Bundle
$
59.95
Google Forms for Special Education – Templates and Tutorials
$
9.99
Teach Organizational Skills to Students
$
5.00
Sensory Processing Resources Handout Pack
$
5.99
Sensory Strategies Workbook
$
17.00
Self Regulation Workbook – Learn About Yourself
$
19.00
Roll a Situation Self-Regulation Activity
$
6.00
Pushing Into the Classroom: Practical Strategies for Pediatric Therapists – Webinar
$
74.97
Emotional Regulation Visuals – Slide Deck
$
5.00
Telehealth Fine Motor Assessment – Functional Skills
$
15.00
Special Edition for Kids with ASD – Recommendations for Kids Who Struggle to Write
$
19.95
Occupational Therapy Awards and Certificates for Children
$
3.00
How to Reduce Screen Time for Kids Ebook
$
14.99
Meal Time Rubrics
$
5.99
Sloth Coloring Pages and Activity Book
$
5.00
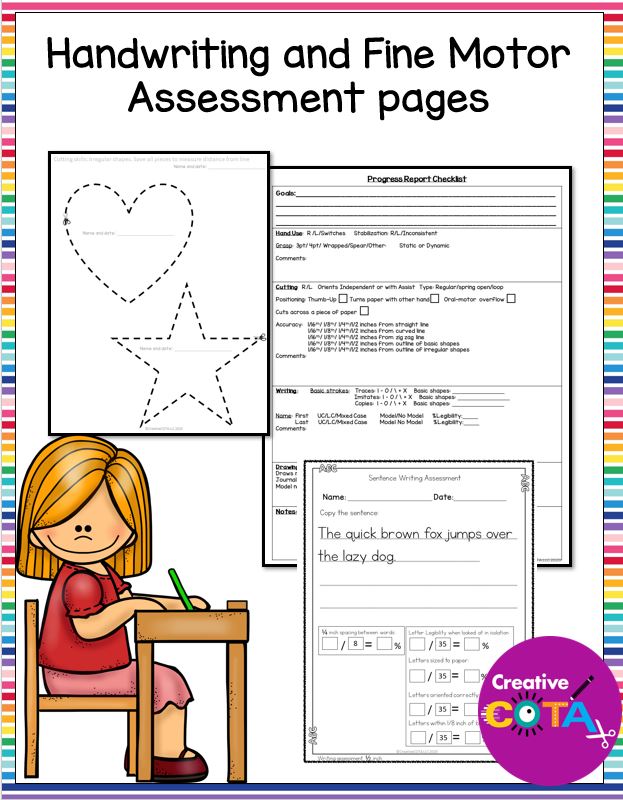
Handwriting and Fine Motor Assessment
$
10.00
Sensory Strategies for the Classroom Bundle
$
62.88
Wiggle Worms: A Guide to Alternative Seating for the Classroom
$
12.99
Clinical Observations at the Park Tool
$
11.00
Get Fit for School Webinar – Popcorn and Animals Make My Muscles Strong!
$
25.00
The Scissor Skills Book
$
15.99
Reflective Journaling for Therapists, Teachers, Parents and Students
$
6.99
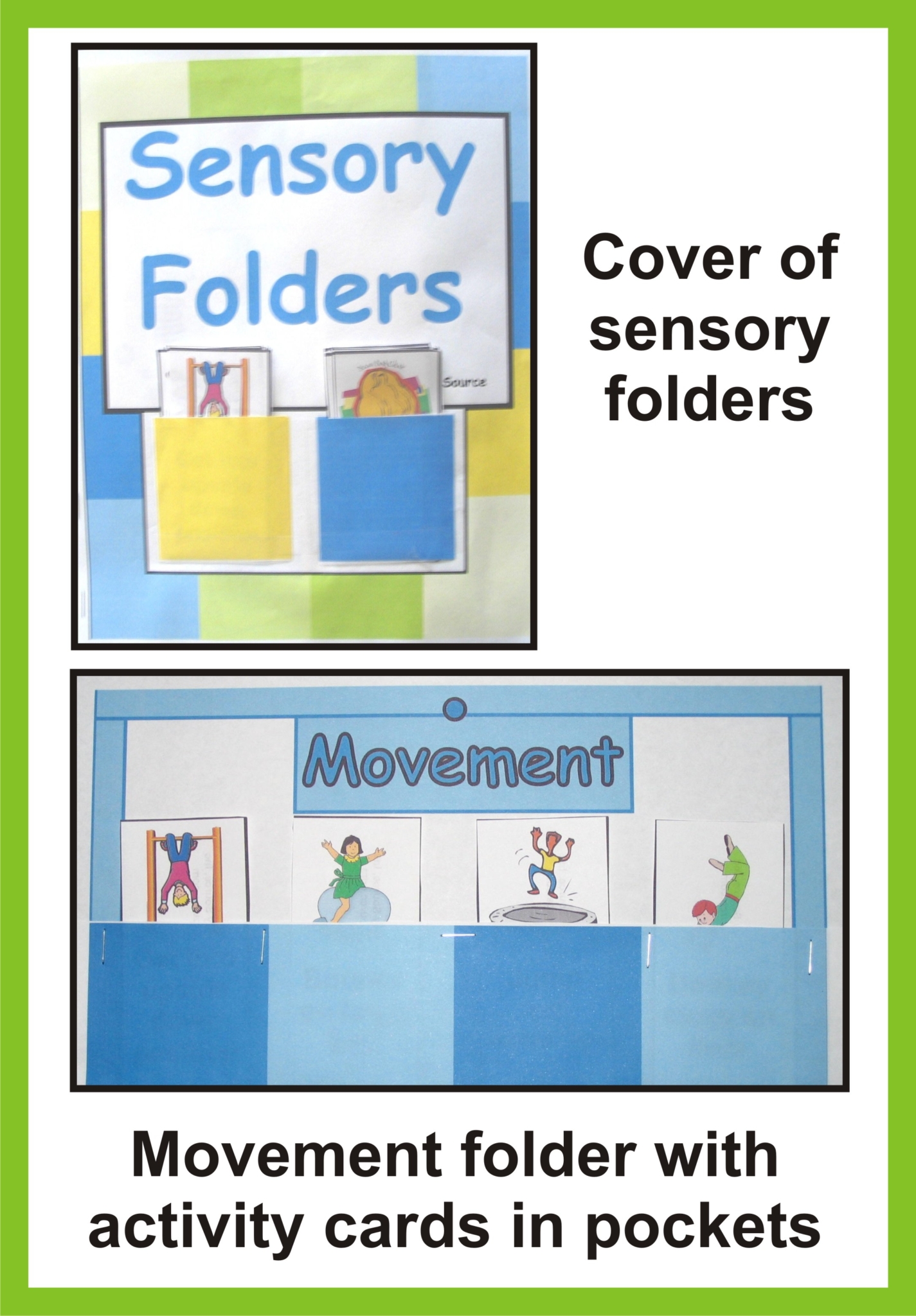
Sensory Folders
$
3.50
Digital Magazine 2026 Your Therapy Source Subscription
$
49.00
Forms and Sheets Data Collection Bundle
$
44.95
Dominant Hand Screener
$
5.00
Occupational Therapy – Complete Set of Visuals
$
5.00
Goal Sheets for Students
$
7.00
School-Based Occupational Therapy Kit
$
75.00
Digital Magazine 2025 Your Therapy Source Subscription
$
59.00
Occupational Therapy Elementary Activities SET TWO Weeks 7-12
$
12.50
Productivity and Time Management Planner
$
19.99
Occupational Therapy Screening IEP Goal Tracking
$
12.50
Sensory Tools Visual Supports
$
12.00
Sensory Lifestyle Handbook
$
19.99
School Routine Checklists in Google Forms
$
9.99
Social Emotional Skills Checklist
$
9.95
Emotional Intelligence Activities for Teens
$
7.00
Guide to School Based Physical Therapy
$
7.99
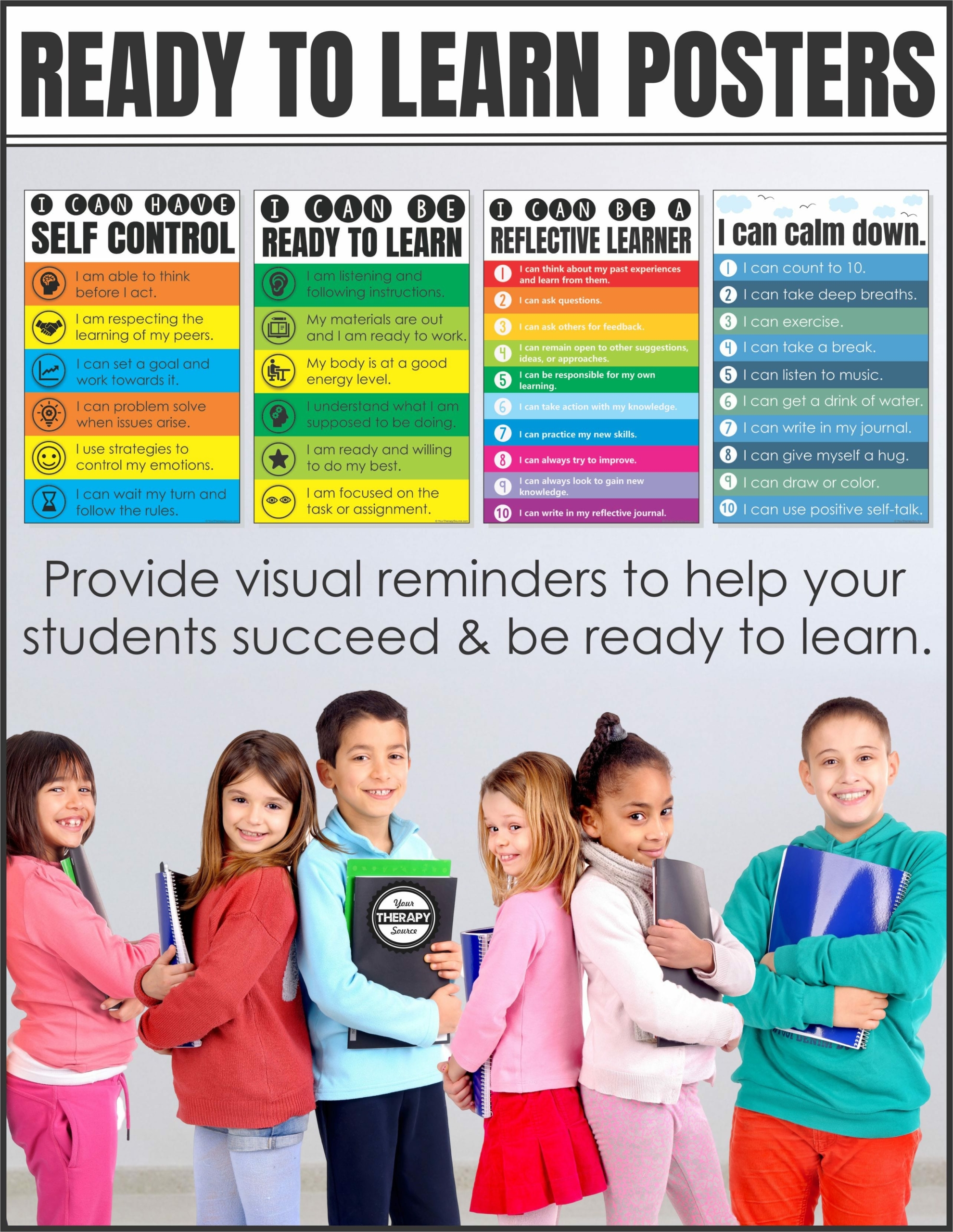
I Can Posters – Help Students Be Ready to Learn
$
4.99
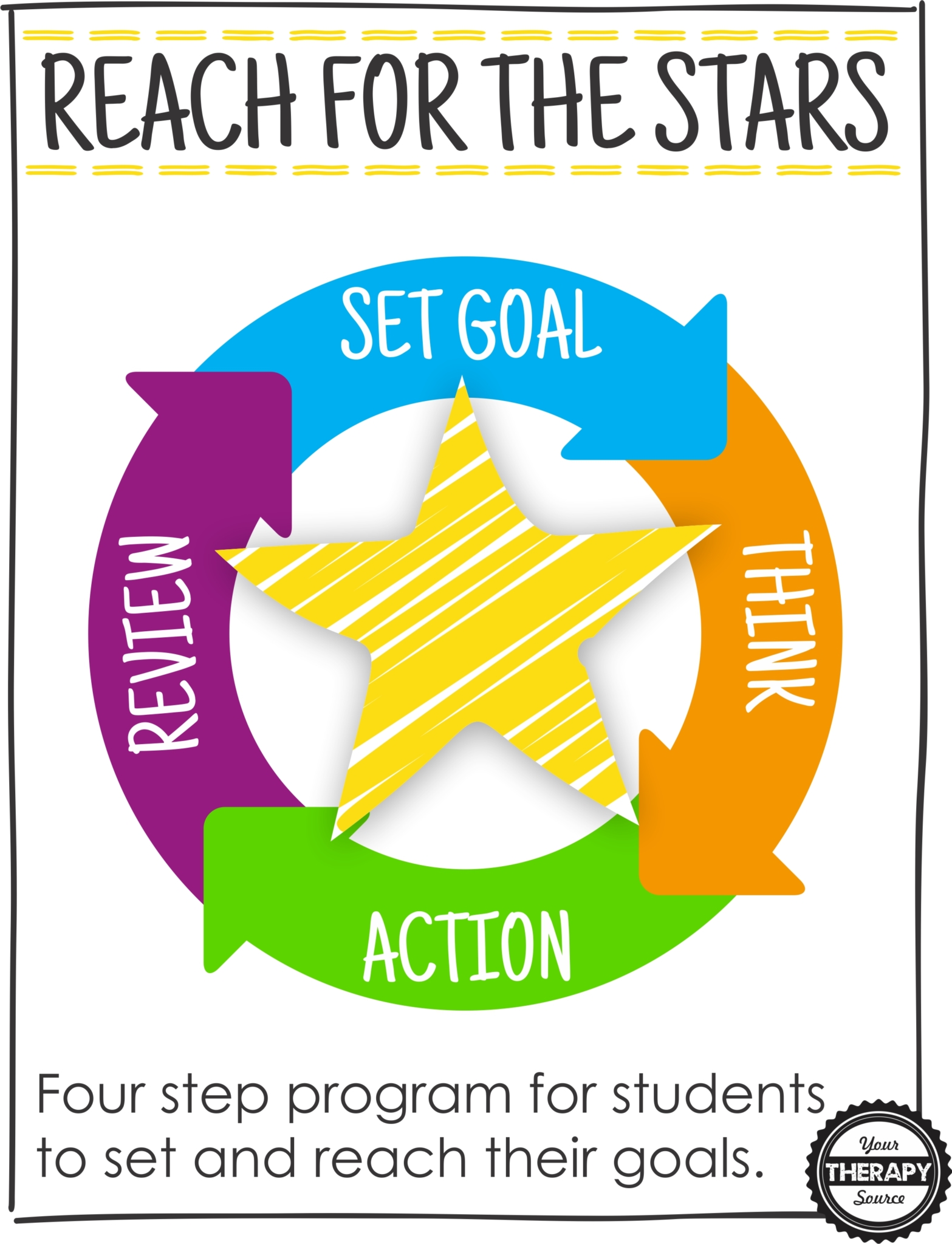
Goal Setting for Students PDF – Reach for the Stars
$
9.95
Self-Advocacy for Students
$
19.95
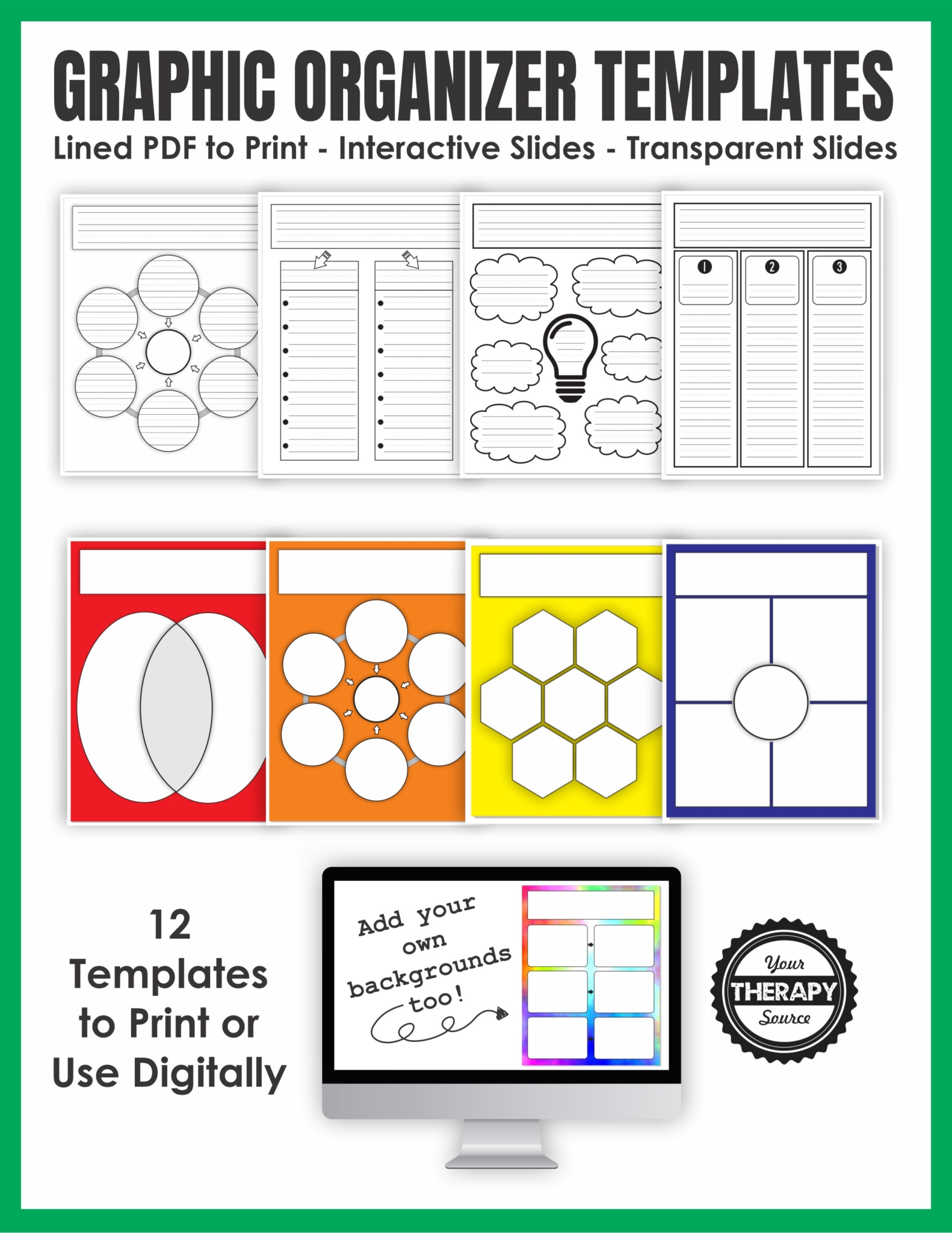
Graphic Organizer Templates – Print and Digital
$
8.00
T.W.O. Tool – Toe Walking Observation Screening Tool
$
9.95
School Based Occupational Therapy Forms
$
13.95
–
$
19.95
Price range: $13.95 through $19.95
JointSmart Child BUNDLE
$
40.97
Guide to School Based Occupational Therapy
$
7.99
Prewriting and Scissor Skills 12 Month Bundle
$
21.00
Self-Regulation Videos and Flash Cards Bundle
$
110.00
Response Board for Therapy Sessions
$
0.99
Autism Sleeps™
$
29.95
School Based Therapy Planner 2024 2025
$
12.99
Early Intervention Occupational Therapy and PT Handouts
$
14.99
JointSmart Child: Living & Thriving With Joint Hypermobility
$
15.99
Physical Therapy Awards and Certificates for Children
$
3.00
Basics of Fine Motor Skills – Developmental Activities for Kids
$
14.99
Sensory Processing/Integration Collection
$
21.21
–
$
29.70
Price range: $21.21 through $29.70
Coleman Curriculum for School Based Occupational Therapy
$
19.95
Positive Affirmations for Students
$
6.99
Hypermobility in Children – The School Years
$
15.99
Fun Emotional Intelligence Activities for Kids
$
7.00
Occupational Therapy UPPER ELEMENTARY SET 2
$
12.50
Creative Pediatric Treatment Strategies Based on the Evidence – Webinar
$
44.97
Vestibular Groove – Explore How Movement Feels
$
7.00
Emotional Regulation Strategies – Animal Theme
$
6.00
School Based Occupational Therapy Forms DOWNLOAD for Printable Forms and Computer Fill In Forms
$
19.95
Reflection Sheet for Behavior – Social Emotional Learning
$
5.00
Meet the Neighbors – Emotional Regulation Activity
$
5.00
Prewriting Success Handout Pack
$
14.99
Sensory Motor Visuals for the Classroom and Home
$
8.75
Calm and Strong: Songs for Self Calming
$
12.00
Tai Chi for Children
$
15.00
Star Charts, Incentive Visuals, Token Boards-Behavior Management for Home BUNDLE
$
10.99
Sensory Mini Books and Charts
$
8.99
Trauma-Informed Therapist Handout Pack
$
14.99
School Based Therapy Planner 2025 2026
$
12.99
RENEW – Digital Magazine 2026 Your Therapy Source Subscription
$
39.00
Occupational Therapy Lesson Plans for 52 Weeks
$
300.00
Fine Motor Data Collection BUNDLE – JAN-DEC Color, Cut, Glue, Write
$
108.00
Original price was: $108.00.
$
15.00
Current price is: $15.00.
Sale!
The Mindful Classroom: Songs and Reflections for Students
$
7.00
Interoception and Emotional Awareness PDF
$
6.00
Healthy Habits for Kids Workbook
$
14.00
Handwriting Success Handout Packet
$
14.99
Emotions Word Search and Activities Packet
$
5.00
Where is the OT, PT or Speech Clip Charts
$
1.00
Sensory Path for Young Learners DIGITAL VERSION
$
19.00
OT Goal Bank and Accomodations
$
7.00
Going to Doctor Visual Schedule, Social Story Starters, Pretend Play, Role-Play
$
2.99
Identifying Emotions for Kids PDF
$
9.00
OT Back to School Telehealth or Distance Learning Slide Decks
$
9.00
Brain–Body Regulation Mega Pack (2026 Edition)
$
181.98
Original price was: $181.98.
$
36.00
Current price is: $36.00.
Sale!
Roll a Sentence
$
5.00
Mindful Kids in 10 Minutes a Day – PreK to 2nd Grade
$
19.95
Documentation Manual for School-Based OT Providers
$
19.99
Emotional Regulation Tracker – Google Sheets
$
14.95
Sensory Path Obstacle Course
$
12.00
A to Z Coping Skills PDF
$
5.00
Emotional Regulation Skills DIGITAL version
$
12.99
School-Based Therapist Handbook Webinar
$
54.97
Brain Training Posters DIGITAL Version
$
9.99
New Year OT Boom Cards
$
6.00
Raising Self Regulated Kids Issue #1 – The Science Behind Self Regulation
$
15.00
Following Directions Bundle
$
55.00
Mindfulness Middle School Workbook
$
19.95
Telehealth 101 – Tips for Implementing Pediatric OT Telehealth
$
24.95
Joint Smart Child Volume 1 + Toilet Training Low Muscle Tone Bundle
$
18.99
RPT: Reminders for Physical Therapy
$
4.99
5 Minute Meditation for Kids – Calming
$
4.99
Visual Schedule Cards
$
14.00
Occupational Therapy Preschool Activities Set 2 – Weeks 7-12
$
12.50
Pediatric Occupational Therapy Training and Mentoring – Step By Step Guide
$
19.95
BrainWorks Online Membership
$
45.00
5 Textured Sensory Stickers
$
5.00
Emotion Board Games
$
6.00
YTS Action Toolkit Annual License
$
99.00
Social Emotional Digital Spinners
$
6.00
Conflict Resolution Task Cards and Self Reflection Questions
$
6.00
Mindful Exercises for Students
$
10.00
Interoception Guide – Listening to Your Body
$
12.00
More Winter OT Boom Cards
$
6.00
School Based Therapy Planner 2026 2027
$
12.99
Occupational Therapy Evaluation Lists and Examples
$
6.00
Developmental Movement Adventures
$
10.00
The Scale of Sensory Strategies (S.O.S.S.) Tool Kit™
$
99.00
Sensory and Self-Regulation Toolkit: OT-Approved Strategies for Kids
$
19.99
What If I Worry Packet
$
6.99
Emotions and Feelings Scrambled Sentences
$
8.00
Small Steps, Big Impact: EBook
$
27.00
Documentation for Early Intervention Pediatric OT
$
19.99
My Sensory Choices Glyph Packet
$
6.00
Therapeutic Activities Using Recycled Materials Masterclass
$
49.00
Pediatric Caregiver Interview Cheat Sheet
$
5.00
The Practical Guide to Toilet Training Your Child with Low Muscle Tone – 2nd Edition
$
26.99
School Based OT Webinar Outside of the Box: More Effective, More Efficient, More Practical and Fun
$
300.00
Feeling Angry and Scared CBT Packet
$
5.00
Positive Affirmation Word Search PDF
$
12.00
Early Elementary Occupational Therapy Weeks 13 to 18
$
12.50
Calming Coloring Mural
$
4.99
Feeling Nervous
$
6.99
Developmental Coordination Disorder Webinar
$
54.97
Self-Regulation Coping Strategies Coloring Pages
$
6.50
Kids and Sleep Handout Packet
$
14.99
Coping Skills Alphabet and Bingo Boards
$
6.50
Coregulation Reflections Audio & Worksheet Bundle
$
7.00
Self Regulation Brain Breaks
$
10.00
The Gifted Child Handout Packet
$
14.99
Meltdowns, Transitions, and Sensory Lifestyle Bundle
$
50.00
Parenting Principles – Ebook and Workbooks
$
29.95
Occupational Therapy Older Elementary Students Weeks 13-18
$
12.50
Shapes of Stillness: A Calming Neurographic Art Series
$
9.00
Mindfulness Activities for the Classroom Grade 3-5
$
19.95
Visual Schedules for Homeschool and Distance Learning EDITABLE
$
3.99
Brain Body Reset
$
12.00
Adult Sensory Processing Preferences for Roommates
$
5.00
SEL in the Classroom Toolkit
$
29.95
Original price was: $29.95.
$
19.95
Current price is: $19.95.
Sale!
Daily Routine Cards
$
12.00
Movement and Mindfulness Curriculum Instant Download
$
220.00
Executive Function Observation Checklist
$
12.00
Guiding Growth: Scaffolding Functional School Skills
$
14.00
Emotion Puzzles
$
5.00
Fall Social Emotional Learning Emotions Bingo
$
8.00
Self Esteem Journal for Kids + Ebook
$
19.00
Calming Card Deck
$
6.00
Cutting Made Simple Course
$
50.00
Shoe Tying Made Simple Course
$
200.00
Healthy Habits for Educators
$
99.95
Teens with Hypermobility and Dysautonomia Handout Packet
$
14.99
Spot the Difference Emotion Cards
$
5.00
Cognitive Exercises – MPower Games
$
24.97
Issue #3: Building Emotional Balance
$
15.00
Assessment of Handwriting Function
$
113.00
Summer Interoceptive Awareness
$
6.50
Winter Activities for Kids Ebook
$
12.00
Calm Down Yoga for Kids
$
45.75
Book Companions for Perspective Taking and Emotions Vocabulary
$
6.00
Print and Cursive Handwriting Rubric Bundle
$
14.50
Autism Feeding Issues – MealSense Program
$
39.99
Social Emotional Learning PDF Starter Pack
$
59.75
Spanish Core Strengthening Exercise Program
$
15.99
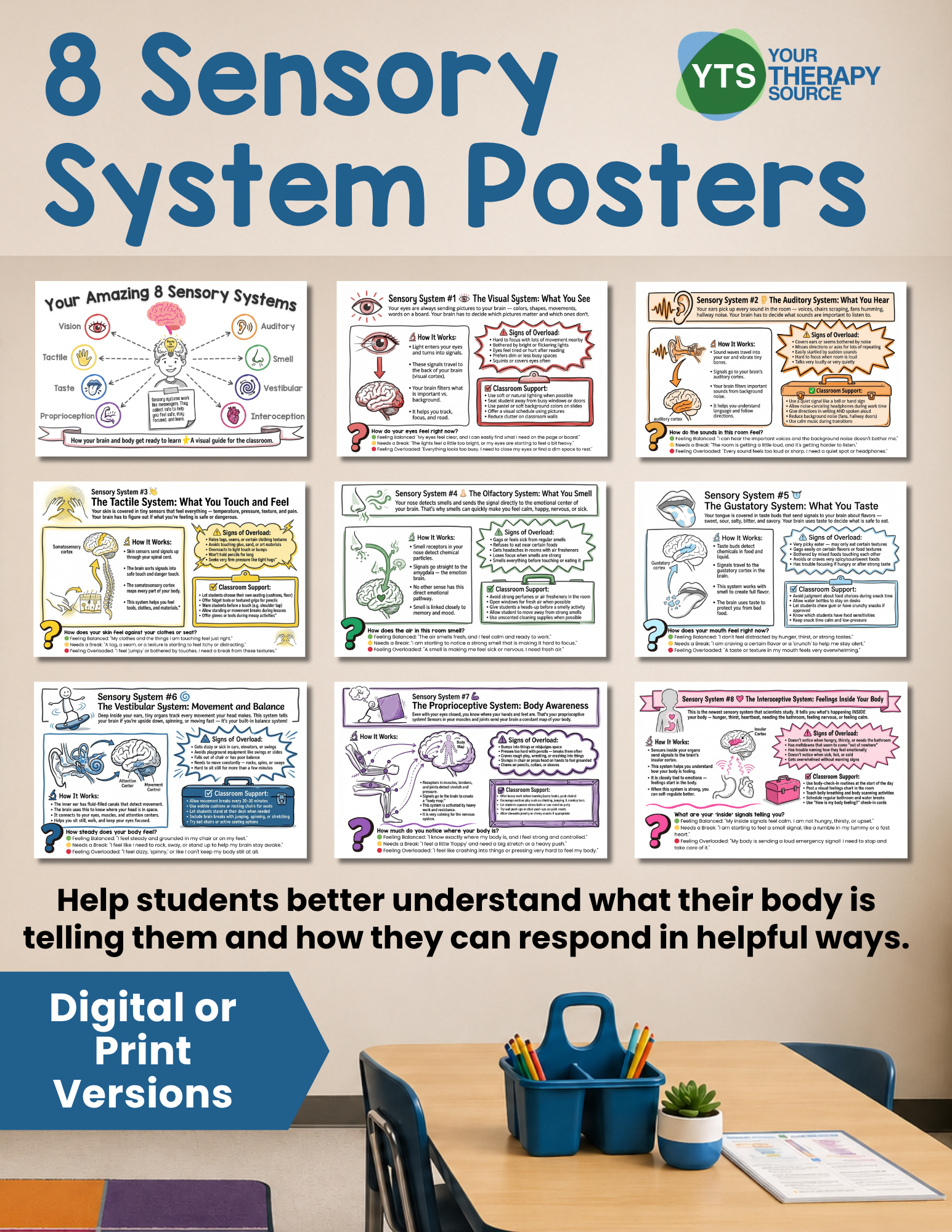
8 Sensory Systems Poster Set – Digital Download
$
17.00
Issue #2 – Self Regulation in a Busy World
$
15.00
Mindfulness for Adults Bundle
$
67.75
Preschool Occupational Therapy Weeks 13-18
$
12.50
Play Based Learning and Therapy Activity Lists
$
10.00
Butterfly Bellies Self-Regulation Bundle
$
23.00
Problem Solving Bundle
$
5.00
Kitchen Skills Success Packet
$
17.99
Back to School Emotions Coloring and Writing
$
7.00
The School-Based Therapist’s Self Assessment Guide
$
24.95
Ghost Occupational Therapy and Speech Packet
$
8.00
Mindful Minutes
$
5.00
Perspective Taking and Emotions Vocabulary Book Companions
$
6.00
Post Covid-19 Pediatric Therapy Implications Course
$
45.00
Breathing Exercise Cards For Kids – Digital Version
$
9.95
Food Theme Fine Motor Data Collection
$
9.00
Spanish Version – Core Strengthening Handbook
$
18.99
Feel, Try, Learn Activities – Digital PDF
$
14.00
Issue #4: Real-Life Case Studies & Practical Examples for Self-Regulation Success
$
15.00
Handout Bundle from Cathy Collyer OTR
$
152.90
Using a Strengths-Based Approach to Behavior
$
197.00
Fantastic Fingers® Fine Motor Program Multi-User License
$
135.00
Habit Trackers for Kids
$
7.99
Original price was: $7.99.
$
5.99
Current price is: $5.99.
Sale!
Self Regulation Workbook PRINT edition – Learn About Yourself
$
19.00
Feelings and Emotions Color and Write
$
8.00
OT Skill Building Monthly Bundle
From:
$
16.00
Original price was: $16.00.
$
12.00
Current price is: $12.00.
Sale!
Student Agency Workbook
$
17.00
Emotional Regulation Activities for Kids – Yoga Bundle
$
158.25
Halloween Emotional Development Packet
$
5.00
Calming Yoga Cards for Kids
$
9.95
St Patrick’s Day Fine Motor Data Collection
$
9.00
Mindfulness Activities and Puzzles
$
7.00
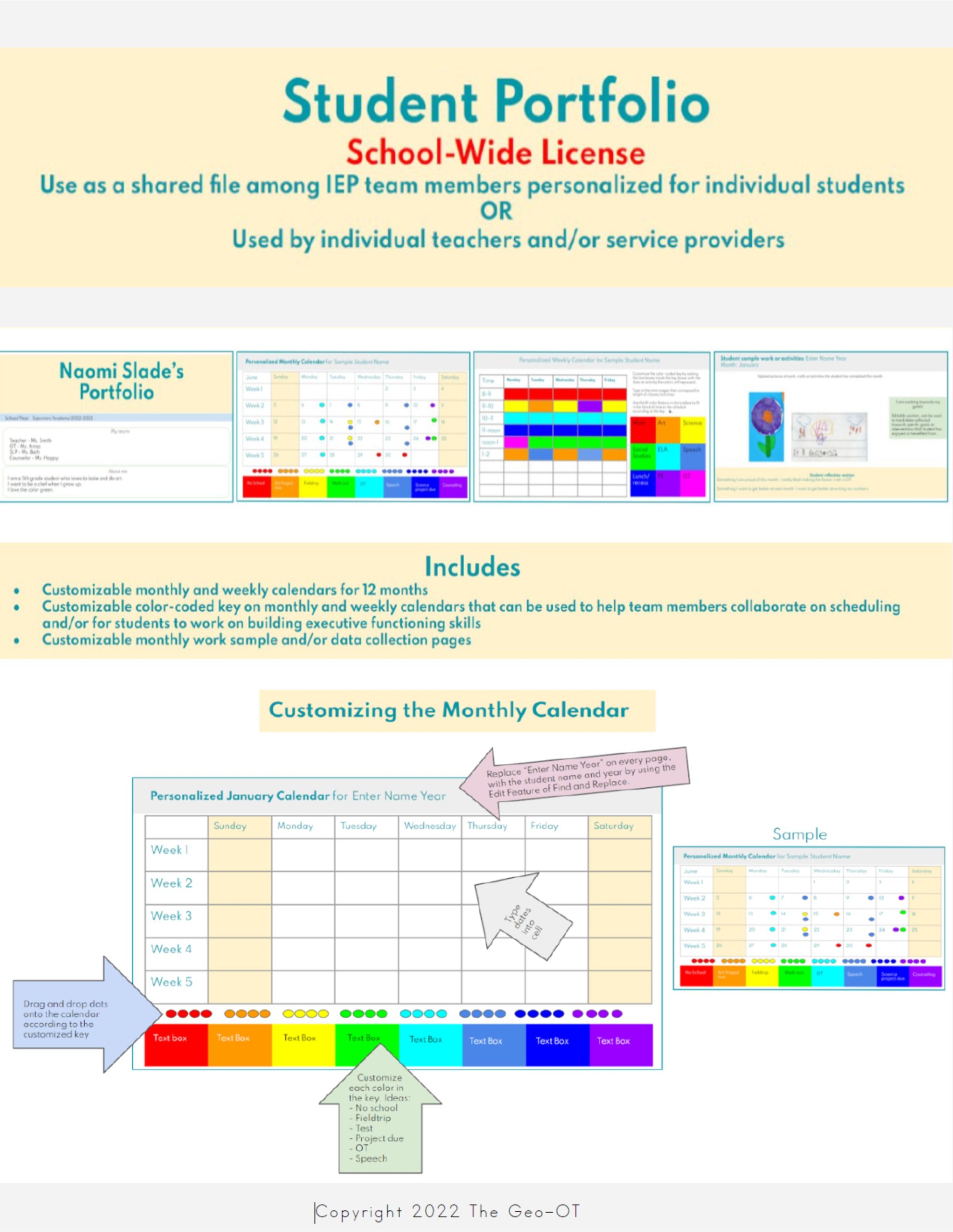
Student Portfolio – SCHOOL WIDE LICENSE
$
19.00
Scissor Skills Success Handout Pack
$
14.99
Social Emotional Sports Bingo
$
9.50
Thriving in Youth Sports
$
21.00
Winter and Christmas Emotions Bingo Games
$
8.00
My School Journal
$
14.95
–
$
15.95
Price range: $14.95 through $15.95
Raising Self Regulated Kids Complete Series Issues #1-4
$
60.00
Spring and Summer Emotions Bingo Game
$
12.00
Brain and Sensory Foundations Course
Scroll to top